Primary cancers of the bones
Commonly known as bone sarcomas, osteosarcomas and chondrosarcomas are the two most prevalent variants. These conditions can affect individuals of all ages, but particularly those in their 20's and 60's.
Managing these conditions presents challenges centred around the removal of tumours in a manner that prevents recurrence. Reconstructing the structure is essential to replace the missing anatomical component and restore function.
Reconstruction generally involves either biological or prosthetic approaches. Biological solutions offer the advantage of reconstructing the missing structure using biological materials and host bone, providing virtually lifelong durability. However, these methods can result in donor site morbidity and a relatively high early complication rate.
The prosthetic approach involves replacing joints and segments with metal implants, enjoying high patient acceptability and good function, but they are subject to wear (Figure 1). Our service uniquely combines both approaches, offering the most appropriate one for specific cases. We have contributed pioneering work in this field, with over 30 years of research dedicated to developing innovative solutions to the problem. Additionally, we operate our own in-house bone bank—the only one of its kind in Singapore.
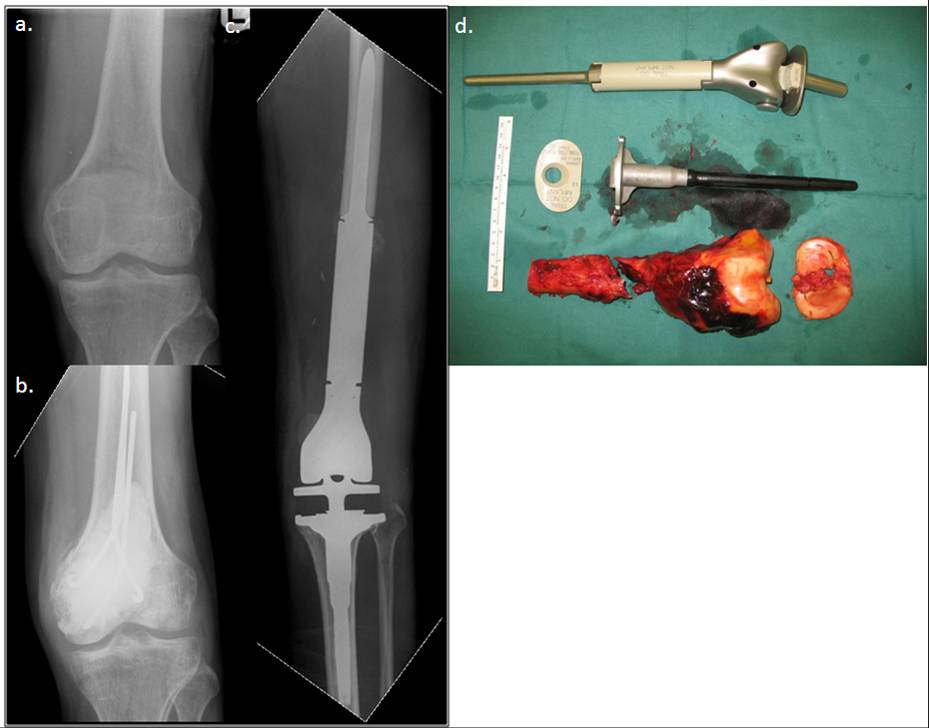 Figure 1. The patient had an osteosarcoma of the lower femur (a). This was biopsied and stabilised and the patient underwent chemotherapy for nine weeks (b).
Figure 1. The patient had an osteosarcoma of the lower femur (a). This was biopsied and stabilised and the patient underwent chemotherapy for nine weeks (b).
The tumour was then resected with oncological sound techniques (the margins of resection were clear of tumour) and reconstructed with a tumor megaprosthesis (c). The tumour was replaced with a prosthesis which resembles the lost bone (d). The patient was able to bear weight and walk soon after surgery.
Primary cancers of the soft tissues
Referred to as soft tissue sarcomas, liposarcomas and malignant fibrous histiocytomas, these occur more commonly in adulthood, whereas rhabdomyosarcomas and synovial sarcomas are predominant in childhood.
The orthopaedic oncologist exhibit a distinctive skill in primarily resecting these tumours to preserve life and, secondarily, reconstructing defects in a way that sustains function. Moreover, these resections are performed to facilitate radiation therapy, a common approach used in managing these conditions (Figure 2).
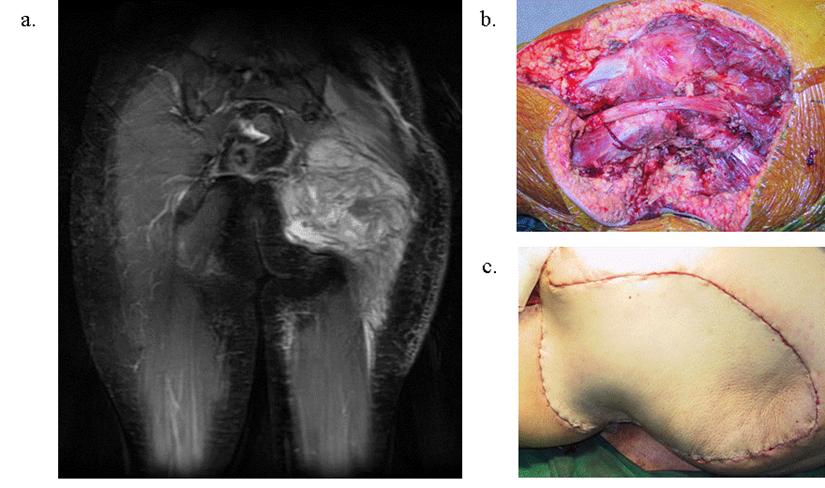 Figure 2. The tumour recurred after two previous resections in a non-musculoskeletal oncology specialised unit in an overseas centre (a). The patient was seen in our unit for a second opinion. We resected the tumour and, using advanced multidisciplinary techniques, were able to replace the lost part in a cosmetic fashion (b) without oncological compromise (margins were clear of tumour (c))
Figure 2. The tumour recurred after two previous resections in a non-musculoskeletal oncology specialised unit in an overseas centre (a). The patient was seen in our unit for a second opinion. We resected the tumour and, using advanced multidisciplinary techniques, were able to replace the lost part in a cosmetic fashion (b) without oncological compromise (margins were clear of tumour (c))
Metastasis
When cancers from other parts of the body spread to the bone and soft tissues, these structures are compromised. Consequently, patients experience non-healing fractures, leading to decreased mobility. This, in turn, diminishes their life expectancy.
Our specialists are trained to reconstruct these affected bones and joints, enabling patients with such conditions to live out their remaining lives with dignity (Figure 3). Additionally, our staff is particularly attuned to the sensitivity required in caring for these patients.
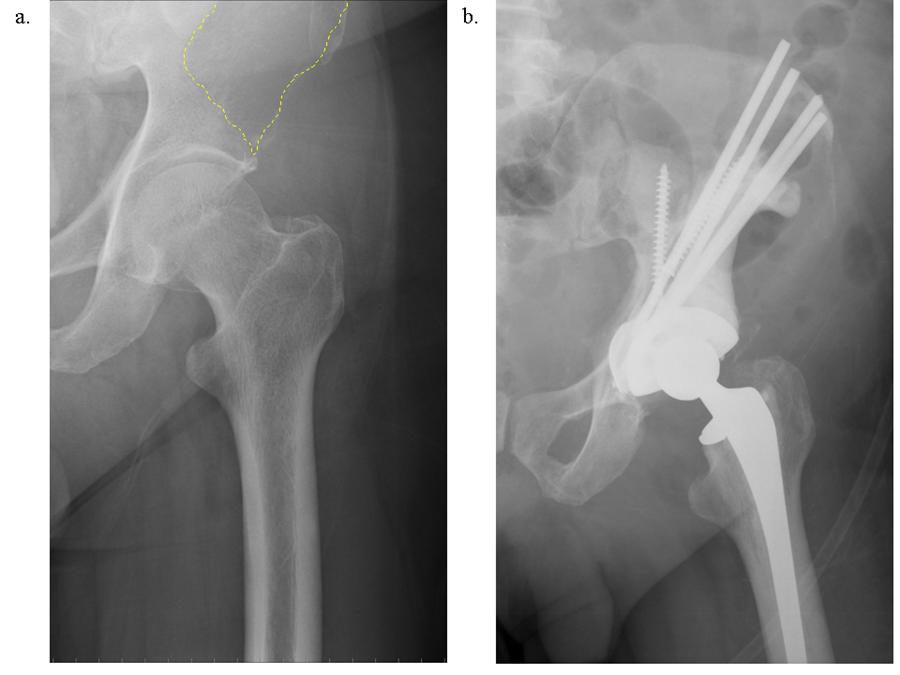
Figure 3. The patient had bladder cancer but was resected. Subsequently, he developed left hip pain and was diagnosed with metastasis to the hip (shown by the dotted area in (a)). Historically, this condition was managed with wheelchair ambulation and radiation. However, we were able to offer new techniques which involve resecting these tumours and replacing the affected joints, allowing the patient to maintain ambulation (b).
Benign tumours of the bones and soft tissues
These conditions are commonly encountered and managed by general orthopaedists and surgeons. Our particular expertise in this field addresses two primary challenges presented by these conditions.
First, diagnosing these conditions presents challenges as they can mimic more severe conditions like cancers. We collaborate closely with the Departments of Pathology and Radiology, engaging in regular meetings to thoroughly discuss such cases before surgical intervention. This approach minimises the risk of misdiagnosis.
Subsequently, when these conditions compromise function and necessitate surgery (e.g. weakening the bone to the point of potential fracture), we are able to reconstruct these conditions with minimal functional impact (Figure 4).
 Figure 4. The patient had a benign condition of the femur, initially overlooked. Typically, most such conditions are managed by general orthopaedists in the early stages, where effective control is feasible. However, when they progress to the point of anatomical disruption within the femur, limb salvage becomes a challenging process (a). Using various advanced techniques, including bone from our in-house bone bank and the selection of metals in implants that do not interfere with subsequent MRI surveillance for recurrent disease, we were able to restore the femur's anatomy.
Figure 4. The patient had a benign condition of the femur, initially overlooked. Typically, most such conditions are managed by general orthopaedists in the early stages, where effective control is feasible. However, when they progress to the point of anatomical disruption within the femur, limb salvage becomes a challenging process (a). Using various advanced techniques, including bone from our in-house bone bank and the selection of metals in implants that do not interfere with subsequent MRI surveillance for recurrent disease, we were able to restore the femur's anatomy.